Exploring the New Forms of Carbidopa/Levodopa with Dr. Vaou

On a recent episode of APDA’s Dr. Gilbert Hosts, I spoke with Dr. Okeanis Vaou, a movement disorders specialist, about the various new formulations of carbidopa/levodopa that are available, including Crexont® and Vyalev®, among others.
Carbidopa/levodopa is the mainstay of treatment for Parkinson’s disease (PD) and is the most effective medication available for PD. Over time, many formulations of this medication have been developed which can make it confusing for people who are trying to understand which version of the medication is best for them.
We covered a lot of ground during the broadcast and Dr. Vaou answered many questions from the audience. (Just click the video below to view the full program). In this article we will address some of the additional audience questions that we did not get to during the broadcast.
For your convenience, we listed the topics and questions from the episode below with timestamps so you can skip to what interests you most.
Video Timestamps
2:31 Dr. Vaou’s presentation about carbidopa/levodopa
23:31 What is ON and OFF time?
26:32 With all of the carbidopa/levodopa options, how do you decide what to prescribe for a particular patient?
29:02 Dietary protein can interfere with the absorption of carbidopa/levodopa. Is there a difference in the protein effect with the various carbidopa/levodopa options?
32:51 If somebody is nauseous from carbidopa/levodopa, what can be done to help them better tolerate the medication?
36:06 For some people, carbidopa/levodopa does not relieve tremor. What can be done to address that?
37:31 If a person has mild PD symptoms, when should carbidopa/levodopa be started?
39:29 Can muscle cramps be a side effect of carbidopa/levodopa? What is the best way to treat cramps?
41:48 What is your opinion on Mucuna pruriens (a legume that contains levodopa)?
43:07 Does carbidopa/levodopa treat balance issues and difficulty walking?
45:08 Does carbidopa/levodopa treat speech difficulties?
46:45 How do people decide whether to take carbidopa/levodopa since it can cause dyskinesias?
49:37 With the two new options of carbidopa/levodopa delivery, should I bring up a potential change in medication with my neurologist?
52:15 If carbidopa/levodopa doesn’t seem to be effective, should I try stopping it?
54:02 When should I consider decreasing my medication?
We have a wealth of additional information on our website about carbidopa/levodopa:
- Common questions about carbidopa/levodopa
- Levodopa dosing and food intake
- Five myths about levodopa
- Additional levodopa related questions
Additional Carbidopa/Levodopa Questions
Here are some additional audience questions that we did not have enough time to answer during our Dr. Gilbert Hosts broadcast with Dr. Vaou:
Q: I have nightmares from carbidopa/levodopa. What should I do?
A: Vivid dreams and nightmares are common side effects of carbidopa/levodopa. One strategy is to refrain from taking the last dose of carbidopa/levodopa close to bedtime and instead take it at least four hours before bedtime. Often this is enough of a change to prevent nightmares. Always let your doctor know if you’re experiencing a new or troublesome symptom so they can help you make adjustments.
Q: Do you have any guidance on how to adjust carbidopa/levodopa and dopamine agonists to reduce hypersexuality or gambling urges?
A: Hypersexuality and gambling are two potential manifestations of impulse control disorders, a set of behavioral abnormalities in which a person is unable to control urges or compulsions. These can be side effects of any dopaminergic medication, but dopamine agonists (including pramipexole, ropinirole, and rotigotine) are most likely to cause them.
Adjusting medications is the first line of treatment for this problem, and this may involve tapering off of dopamine agonists or decreasing other dopaminergic medications.
- Lowering medication can be challenging because dopaminergic medications are needed to treat the movement aspects of PD.
- Stopping PD medications altogether is usually not possible, since the person with PD needs the medication to allow them to move. However, stopping or reducing the dose of the dopamine agonist can help.
When lowering or stopping a dopamine agonist, care must be taken not to cause a withdrawal syndrome. Dopamine agonist withdrawal syndrome (DAWS) occurs when a dopamine agonist is lowered or stopped too quickly and its symptoms include irritability, depression, and even suicidality. People with PD and their care partners should therefore be warned about the possibility of withdrawal when the dose of a dopamine agonist is lowered. Tapering the dose must be done very slowly and with the guidance of your neurologist.
Q: Is being very tired a side effect of carbidopa/levodopa or just Parkinson’s, or both?
A: Both! Fatigue can be a side effect of carbidopa/levodopa and can also be due to PD itself. Sometimes it is very hard to tease out which is which, so keeping a diary can be helpful in which you record when you take your medication and when you have a particular side effect. If there is a relationship between the timing of medication and a particular symptom, then adjusting the timing of the doses or the amount of the medication taken may be helpful. Be sure to talk to your doctor about any symptoms you’re experiencing and seek their guidance before making changes to your medication schedule.
Q: If a patient is no longer receiving enough benefits from their current dose of immediate-release carbidopa/levodopa, what are the options?
A: Here are three potential options:
- Increase the number of doses or the strength of the dose of the current formulation of carbidopa/levodopa. Change the formulation to one of the newer formulations of carbidopa/levodopa.
- Add another type of medication to enhance the effect of carbidopa/levodopa. Options include an MAOB inhibitor, COMT inhibitor, or dopamine agonist.
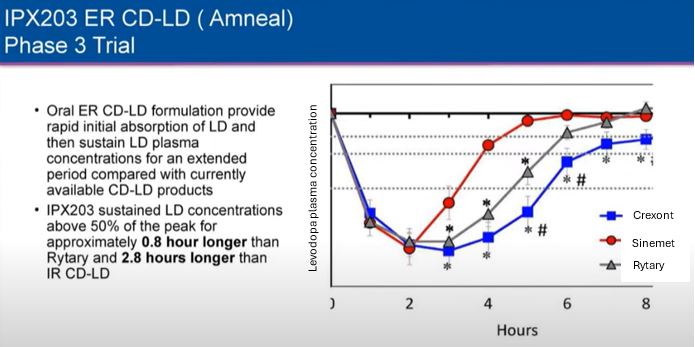
Q: Have Rytary and Crexont been compared to each other? Which is the longest-lasting? Which works better for dystonia? How does protein affect absorption of each?
A: Yes – Rytary and Crexont were compared with regard to how long they each last. Based on the study done, Crexont gives about 0.8 hours more benefit per dose than Rytary and about 2.8 hours more benefit per dose than Sinemet. (see image below) This information was also demonstrated in a poster presentation. To my knowledge, at this time the two medications have not been compared with regard to any other feature, such as protein effect or management of dystonia.
Q: I have not felt an improvement in my symptoms since I started carbidopa/levodopa four years ago. What should I do?
A: Parkinson’s symptoms are comprised of motor symptoms such as tremor, slowness, stiffness, and walking problems as well as a long list of potential non-motor symptoms such as depression, fatigue, sleep problems, cognitive problems, dizziness, constipation, urinary problems, and more. For the most part, carbidopa/levodopa treats the motor symptoms of PD and not the non-motor symptoms.
There are a couple of possibilities in your situation:
- It is possible that you are not on enough medication and taking more would help your symptoms.
- It is possible that the medication you are taking gives you a smooth, sustained response that does not dip between doses. If you are always feeling mild benefit from the medication, then you won’t be able to feel any particular dose kicking in.
- Tremor specifically is sometimes not as responsive to levodopa as other PD symptoms such as slowness and stiffness. Because tremor is so visual, a person may assume that nothing has improved if the tremor stays the same, when in fact they are receiving benefit for their slowness and stiffness from the medication.
- The symptoms that you are hoping to improve are not responsive to levodopa.
- Least likely, but possible, is that you don’t have PD but rather a related condition whose symptoms do not respond to carbidopa/levodopa.
You should talk with your neurologist about all these possibilities as to why you don’t perceive a benefit from carbidopa/levodopa.
Q: If someone has PD, how many days will it take before they see improvement from medication?
A: There is variability in how long it takes for medication to be effective. It makes sense to give a new medication or change in dose of medication about two weeks to work before evaluating whether it is effective or not.
Q: Does carbidopa/levodopa work for reducing anxiety-related tremors?
A: All tremors will get worse when a person is anxious, including a PD tremor. Usually, treating the anxiety is necessary to get that increase in tremor under control.
Tips & Takeaways
- Listen to a very interesting broadcast dedicated to answering your questions about the various forms of carbidopa/levodopa
- Talk with your doctor about whether one of the newer formulations of carbidopa/levodopa is right for you.
- Never stop taking a medication or adjust your dosage without consulting your neurologist first.
- To view all past episodes of Dr. Gilbert Hosts, view the YouTube playlist.
- If you have a PD-related question, you can submit it to our Ask A Doctor portal.