Swallowing Problems and Drooling
Swallowing difficulties in Parkinson’s disease
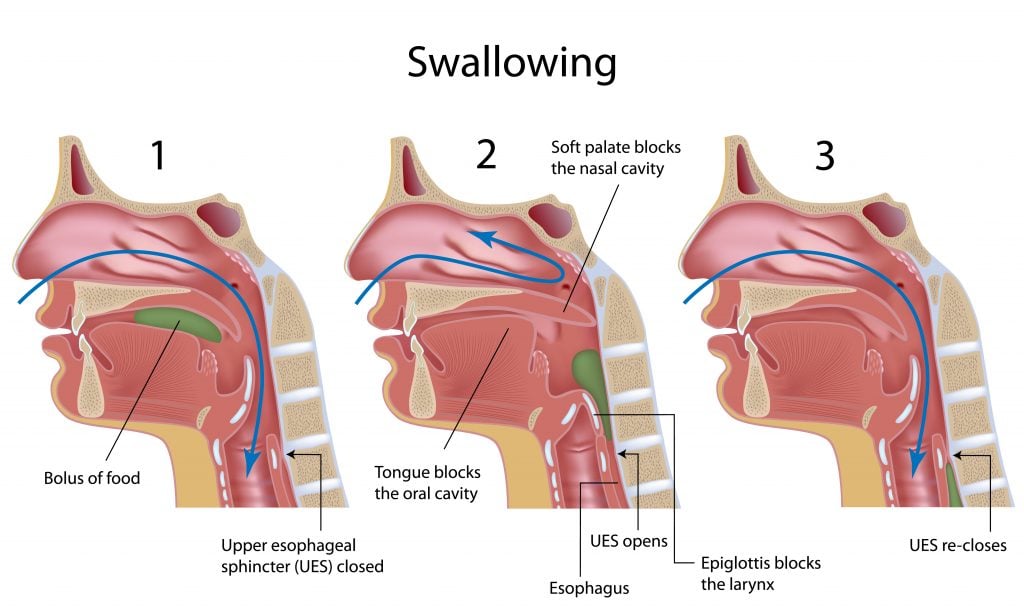
The act of swallowing involves a complex series of activities that begin in the mouth, continue in the pharynx (or the throat) and end in the esophagus. These include chewing, using the tongue to move the bolus of food to the back of the throat and then coordinating the muscles that both propel the food into the esophagus and protect the airway or trachea from food penetration. Swallowing dysfunction (also called dysphagia) can be considered both a motor and a non-motor symptom of PD. Loss of dopamine neurons in the substantia nigra area of the brain can cause the motor dysfunction that impairs swallowing. However, loss of neurons in other areas of the brain, such as the cortex and lower brain stem can also affect the overall control and coordination of swallowing, and can be thought of as a non-motor symptom of PD. Swallowing issues are very important to diagnose. Impacts on your daily life and your health can range from difficulties with meals to more extreme (but less common) cases where it could lead to choking and aspiration which can be very serious or even fatal.
How do you know if you or your loved one has a problem with swallowing?
Swallowing difficulties can start very subtly and initially not be obvious to either the person with PD or their loved ones. There are signs to look out for before swallowing difficulty becomes overt (i.e. choking on food). Some of the signs you should pay attention to include:
- Slow rate of eating – people with difficulty swallowing may slow down their eating in order to avoid coughing or choking
- Fatigue during eating or decreased enjoyment of food
- A sensation that food is “sticking” in the throat
- Coughing or excessive throat clearing during eating
- Difficulty in swallowing pills
- Unexplained weight loss – people with difficulty swallowing may reduce their consumption in an attempt to eat without coughing or choking
- Change in dietary habits – people with difficult swallowing may alter their diet in order to avoid foods that cause difficulty. This may not be a choice made consciously
- Diagnosis of a pneumonia – this could be caused by aspiration, or entry of a foreign substance (i.e. food) into the airway
If you think there might be a swallowing issue, it is important to speak with your doctor about it. There are steps you can take to properly assess the situation (i.e., a swallowing evaluation) and improve your swallowing function. This can in turn reduce your risk of choking, make eating more enjoyable, and lessen the chances of unwanted weight loss and/or other discomforts.
What is a swallowing evaluation?
If because of the above signs there is concern that swallowing difficulties exist, your doctor may recommend a swallow evaluation, which can be performed by a speech and language pathologist.
There are two main ways to evaluate someone’s swallow:
- Modified barium swallow study – This is the most common test that is performed. The person is asked to ingest different consistencies of barium and moving x-rays are taken that follow the barium as it is swallowed. This x-ray video pinpoints the areas of the swallow that are problematic and helps to determine the correct exercises to address the problem.
- Fiberoptic endoscopic evaluation of swallowing (FEES) is another type of test that can be performed to evaluate swallow. During this procedure, a very thin flexible fiberoptic tube which is hooked up to a camera and light source, is passed through the nasal passage. The tube does not go down the throat, but allows swallowing to be observed. This procedure is painless and well-tolerated by most individuals.
If you have swallowing difficulty, what can be done?
In some cases, swallowing function varies in response to dopamine medication doses, much like other aspects of motor function. Therefore, if swallowing becomes problematic, an increase in dopaminergic medications can be tried. In addition, make sure you undergo a swallow evaluation when you are in the ON state.
Even before a formal swallow study, you can take steps to increase the efficiency of your swallow. These include:
- Sit upright during all eating and drinking, even when taking pills
- Tilt the head slightly forward, not backward, as you swallow
- Take small bites of food, chew thoroughly, and do not add any more food until everything from the first bite has been swallowed
- Take small sips of liquid
- Concentrate while moving the food backward in the mouth with the tongue
- “Double swallow” (swallow a second time) if the food did not go down completely with the first swallow
- Sometimes taking a sip of liquid between bites of food can help to wash the food down
- If eating is very tiring, try several smaller meals spaced out during the day instead of three large meals.
Swallowing exercises can be very helpful to improve your swallowing
After a formal swallow assessment, swallowing therapy sessions can be designed for you, involving exercises tailored to the specific parts of your mouth and throat that are causing the swallowing problem. Sessions may involve practicing compensatory swallowing strategies with various types of foods in order to maximize safety and efficiency while swallowing.
During swallow therapy, recommendations may include:
- Best feeding techniques
- Exercises to strengthen oral and throat muscles
- Compensatory techniques to assist in safe swallowing
- Oral and mouth care techniques
- Appropriate food selection and ways to modify food texture
- Safe positioning strategies
- Patient/family education
Choosing foods for successful eating
Part of formal swallow therapy will be to make appropriate food suggestions that you can eat safely. Good food choices include:
- Foods that don’t require vigorous chewing. Avoid dry and crumbly foods.
- Moderately textured wheat breads instead of very coarse, nutty breads or very soft, white breads.
- Oatmeal, cream of wheat or moistened dry cereals instead of coarse, dry cereals.
- Well-cooked, tender chicken/turkey, well-cooked fish without bones, chopped and ground meats, instead of stringy, tough meats that require a lot of chewing.
- Soft casseroles and poached or scrambled eggs
- Mashed potatoes or rice, moistened with gravy or margarine, instead of wild rice or French-fried potatoes.
- Soft, cooked pasta elbows, instead of long spaghetti.
- Soft, well-cooked vegetables, cut up or creamed, instead of raw vegetables or those with a hard texture.
- Pureed or mashed fruits, fruit juices and fruit sauces, instead of fruits with seeds or hard outer skins. Avoid nuts, seeds or coconut.
- Custard, yogurt, ice cream or other soft desserts
Drooling & Parkinson’s
Poor control of saliva is known as sialorrhea. This problem may be mild and result in a simple issue such as a wet pillow in the morning. In some cases however, the problem can be severe, and causes excessive drooling. Drooling is not only an annoyance but can result in significant embarrassment and social isolation.
People with PD have problems controlling saliva because the muscles of the oral cavity, face, and neck may have less control than normal and there may be a delay in the person’s ability to trigger a swallow. Sometimes there is excess saliva in the mouth because swallowing is less frequent, due to the general slowness of movement that accompanies PD.
Solutions to drooling
Anti-cholinergic medications such as glycopyrrolate and scopolamine can cause dry mouth and can be useful to control drooling. Unfortunately, because these medications enter the blood stream, they can also cause effects in other parts of the body such as urinary retention, constipation and blurry vision. Scopolamine can also cause cognitive side effects such as drowsiness and confusion. Therefore, these medications need to be used with caution. Some physicians prescribe atropine ophthalmic drops (another anticholinergic medication) to be placed under the tongue to control drooling. This method is meant to deliver the anti-cholinergic effects more locally, thereby preventing the anti-cholinergic side effects in other parts of the body. However, this too must be used with caution as effects can still be widespread and much care has to be taken to deliver only 1-2 drops under the tongue at a time.
Botulinum toxin injections into the salivary glands can decrease production of saliva and thereby decrease drooling. They have become a common and effective method of controlling saliva with minimal side effects.
There are three sets of salivary glands: the parotid glands (in the cheek), the sublingual glands (under the tongue) and the submandibular glands (under the jaw). Parotid injections are the most straightforward and can be performed by most movement disorder physicians during a routine office visit. If these injections are not sufficient to control the drooling however, the next step would be to try botulinum toxin injections of the sublingual and/or submandibular salivary glands. This is a more specialized procedure and may require a visit to an ENT physician.
It is important to note that botulinum toxin not only decreases saliva production but also weakens muscles, including the muscles of swallowing. Botulinum toxin injections are therefore not a treatment for swallow dysfunction and can in fact cause swallow dysfunction. The parotid gland in the cheek is far enough away from the swallowing muscles that impairment of swallow is typically not a side effect, although it can be in rare cases. Sublingual and submandibular salivary glands are in close proximity to the swallowing muscles and injections of these salivary glands therefore have a higher risk of causing swallow dysfunction. Therefore, only someone trained specifically in these injections should perform them.
Tips and Takeaways
- Swallow impairment and drooling are two common symptoms of oral dysfunction in Parkinson’s disease.
- Subtle signs of swallow dysfunction can include slow eating, coughing with eating and weight loss.
- If swallow dysfunction is suspected, a swallow evaluation can pinpoint what the problem is and swallow therapy can help improve it.
- Drooling can be helped by oral medications or injections of Botulinum toxin but need to be used carefully so as not to cause swallowing difficulties.
- Do not suffer silently or wait until the problem is very advanced before seeking help. Talk to your doctor as soon as you notice any issues or potential difficulties so proactive steps can be taken to lessen the impact of swallowing issues or drooling and also to keep you safe and comfortable.